
International Journal of Clinical and Medical Research
ISSN Print: N/A
ISSN Online: 3134-8831
About: International Journal of Clinical and Medical Research (IJCAMR) is an open-access, peer-reviewed journal dedicated to the publication of high-quality research in the field of clinical and medical sciences. The journal aims to provide a platform for researchers, clinicians, and healthcare professionals to share knowledge, exchange ideas, and promote scientific advancement in healthcare.
International Journal of Clinical and Medical Research | Year 2026 | Volume 3 | Issue 1 | Pages 1-15
Herbal Plants and Phytochemicals application in Ulcerative Colitis: Therapeutic Potential and Mechanistic Insights
Shabab Nasir1 , Maryam Farrukh 2* , Yasmeen Fareed3 , Rafia Sadia4 and Ejaz Basheer51,3,4Department Zoology Government College University, Faisalabad, Punjab, 38000, Pakistan
2Department of Pharmacology, Faculty of Pharmaceutical Sciences, Government College University, Faisalabad, Punjab, 38000, Pakistan
5Department of Pharmacognosy, Faculty of Pharmaceutical Sciences, Government College, Faisalabad, Punjab, 38000, Pakistan
View PDF Download XML Download DOI XML DOI: 10.66590/ijcmr2026030101
Abstract
Ulcerative colitis (UC), a chronic inflammatory collapse of the colon, is characterized by dysregulated immune responses, including significant cytokines including interleukins and tumor necrosis factor-α, as well as recurrent mucosal inflammation and decreased epithelial barrier function.Its pathophysiology is highly complex and involves genetic predisposition, environmental stressors, gut microbiota imbalance and immunological dysfunction.UC presents as urges, bloody diarrhea and pain in the abdomen. It develops into moderate inflammation to severe and fulminant disease which can have long-term effects and high risk of colon cancer. Examples of traditional therapy that are effective in the initiation and maintenance of remission include amino salicylates, corticosteroids, immunomodulators, and biologics; however, their use is often limited in the long run due to adverse effects, expense and insufficient mucosal repair. Medicinal herbs and their bioactive phytochemicals have garnered a lot of interest recently as a possible supplemental or alternative remidies for ulcerative colitis because of their anti-inflammatory, antioxidant and mucosal protecting qualities.Flavonoids, alkaloids, and polyphenols found in aloe vera, Boswellia serrata and Camellia sinensis improve mucosal defense, lower oxidative stress and control important inflammatory pathways including NF-κB, MAPK, and JAK-STAT signaling. Phytochemicals like quercetin, apigenin, arctiine, acetyl-11-keto-boswellic acid show potential therapeutic effects by targeting the processes of cytokine generation, immune cell activation, and epithelial repair. The pathogenesis, clinical progression and the existing treatment options of ulcerative colitis (UC) are discussed in this review, as well as the increasing importance of plant-based substances as safer and cost-effective alternatives to manage the disease over time.
INTRODUCTION
Introduction of Ulcerative Colitis
Bloody diarrhea, pus discharge, mucus, and abdominal cramps during bowel movements are the most typical signs of ulcerative colitis (UC), an inflammatory bowel illness that primarily affects the colonic mucosa and sub-mucosa. An elevated long-term risk of colorectal cancer has been associated with IBD. Although the exact origin of IBD is unclear, a complex interplay of host immunological, genetic and environmental variables is believed to be responsible [1]. The pathological findings associated with ulcerative colitis include elevated levels of certain inflammatory mediators, oxidative stress indicators, mucosal dysfunction, abnormal glycosaminoglycan content, decreased oxidation of short chain fatty acids (SCFAs), increased intestinal permeability, increased sulfide production and decreased methylation. High levels of prostaglandin, nitric oxide and other oxidative stress products are produced by the inflamed mucosa in ulcerative colitis [2].
Chronic inflammation damages the intestines permanently and increases the risk of adverse outcomes such as colectomy and colorectal cancer which lowers patient’s quality of life and poses serious social and economic problems, possibly even raising death rates. Presently, there is no cure for the disease and the primary approach to management focuses on alleviating symptoms. The therapy plan is customized to the intensity of the condition leading to individualized adjustments for each patient [3].
There are between 0.6 and 24.3 instances of ulcerative colitis per 100,000 people worldwide. According to a comprehensive analysis of population-based research, the prevalence varies from 1.2 to 57.3 cases per 100,000 in Asia and from 14.5 to 505.0 and 139.8 to 286.3 cases per 100,000 in North America and Europe respectively. The impact is equivalent for men and women. Although UC can appear at any age, it is most commonly identified in the second to fourth decades of life [3].
A mismatch of abnormally regulated cytokines that are both pro-inflammatory and anti-inflammatory is the primary cause of a condition called ulcerative colitis. Ulcerative colitis is brought on and sustained by inflammatory cytokines derived from T cells, B cells and macrophages. Tumor necrosis factor-α (TNF-α), interleukin-1 (IL-1), IL-6, IL-8, the granulocyte–macrophage colony- stimulating factor and converting growth factor-β (TGF-β) represent a few of the pro-inflammatory cytokines that trigger cartilage in the articular region to be destroyed [4].
Amino salicylates, corticosteroids and immunosuppressant medications are instances of conventional therapies for ulcerative colitis (UC) that are generally effective in triggering and maintaining recovery but they frequently cause side effects. Many biomedical drugs including integrin, Janus kinase (JAK) and tumor necrosis factor (TNF) have been designed to address different cellular processes.However, instead of promoting histological recovery, these medications concentrate on the mechanisms of inflammation to halt the progression of the illness and a majority of these treatments are costly for individuals with moderate and modest incomes.Therefore, it is essential to look for UC treatment alternatives that are both cost-effective and have less negative side effects [3]. Since ancient times, plants and their products have been utilized in folklore to cure a range of maladies. Herbal medicine is currently emerging as a promising substitute for synthetic medications that are sold commercially for a variety of illnesses.Within the various biologically active compounds that are prevalent in flora are flavonoids, carotenoids, phenolic acids, alkaloids, terpenoids and additional phytochemicals that possess significant therapeutic properties.These substances' antioxidant, anti-inflammatory, antibacterial and anticancer qualities may alter critical biological mechanisms related to the emergence of disease. Plant therapy is founded on perceptions of effectiveness, availability, affordability and minimal or nonexistent adverse reactions. Several botanical remedies that exhibit gastroprotective properties have been used to alleviate UC, digestive problems and other corresponding ailments until several centuries ago [1].
Medications made from plants work to reduce intestinal inflammation mainly in two ways: either by lowering the release of pepsin and acid, or by supporting cytoprotection through mucosal defense mechanisms. These drugs regulate protective (cellular mucus, mucin synthesis, mucosal blood flow, bicarbonate secretion and cell turnover) and offensive (pepsin, acid, bile salts and H. pylori) elements. Multiple substances derived from herbal products such as cavidine, chelerythrine, quercetin, hesperidin, α-pinene and garcinol have been found to be utilized to manage ulcer problems. Due to their natural origins, patients with ulcers and inflammation are increasingly using natural remedies like plants and herbal derivatives, which have little or no negative side effects. Among the vital herbal components with antiulcerogenic properties are Boswellia acid (Boswellia serrata), arctigenin (Arctium lappa), curcumin (Curcuma longa), gymnemic acid (Gymnema sylvestre), shogaol (Zingiber officinale) and catechin (Camellia sinensis) [5].
Pathology of Ulcer Colitis
Persistent inflammation that arises in the rectum and extends simultaneously proximately is a sign of ulcerative colitis, a permanent irritable bowel disorder. In contrast to Crohn's disorder, the medical condition is mostly limited morphologically to the mucosal and overlying gastrointestinal tract. Inflammation is both cause and an effect of mucosal damage and recent developments have changed our perspective of UC from a purely immune-mediated illness to one that is fueled by host-microbial interactions, immunological dysregulation and epithelial barrier failure [6].
One significant and current concept in UC pathogenesis is the breakdown of the primary epithelial permeability. Enhanced epithelial porosity, impaired tight junction elasticity and poor regrowth of injured epithelium all lead to the lamina propria's inappropriate exposure to luminal antigens.
The mucus layer thins and becomes discontinuous as a result of decreased goblet cell density and changed mucin composition, especially decreased mucin 2. This weakened barrier which predisposes to persistent mucosal inflammation, is now regarded as an early pathogenic event rather than a subsequent one [7]. The mechanism of ulcerative colitis requires multiple inflamed cells that produce various inflammatory cytokines. The immune cells in Peyer's patches, which primarily consist of B cells, T cells (including T follicular helper cells) and dendritic cells are stimulated by foreign antigens detected by the gastrointestinal epithelium's microfolds cells (M cells) [8]. Numerous immune cells create immunoglobulin A When M cells absorb bacterial antigens from the intestinal lumen. This protein binds antigens released by invasive pathogenic bacteria to prevent infection. In the mesenteric lymph nodes, dendritic cells expose naïve T lymphocytes to bacterial antigens. The antigen-expressing young T cells produce pro-inflammatory cytokines that are believed to encourage tissue destruction and persistent inflammation along with anti-inflammatory cytokines that encourage barrier function and the resolution of inflammation after dividing into various subtypes of helper T cells [6]. The infiltration of inflammation in ulcerative colitis is driven by innate immune cells, namely neutrophils, macrophages and dendritic cells. Neutrophilic penetration of the crypt epithelium is responsible for the two main morphological traits of cryptitis and crypt tumors.
Instead of effectively clearing germs, macrophages in UC have a pro-inflammatory phenotype with increased cytokine production [9]. According to recent research, chronicity may be caused by a malfunction in the resolution of inflammation and a breakdown in macrophage-mediated tissue healing. It is now known that adaptive immune responses in UC are more intricate than the traditional Th2 paradigm. Current research shows that IL-23-driven pathways and Th17 cells are involved, bridging innate and adaptive immunity, even if IL-13-mediated epithelium damage is still relevant. The immunological tolerance is further compromised by the dysregulation of regulatory T cells, which permits ongoing inflammation against commensal microbiota [10]. More recent biologics that target IL-12/23 and downstream signaling pathways are effective because of this changing cytokine network. Epithelial apoptosis, immune cell survival and the transcription of inflammatory genes are all maintained at the molecular level by the continuous activation of intracellular signaling pathways such MAP kinase, JAK–STAT (inflammatory gene transcription) and NF-κB. Additionally, these pathways affect fibrosis and epithelial renewal. Although there is less fibrosis and transmural remodeling in UC than in Crohn's disease, long-term illness-related architectural distortion such as crypt branching, shortening and basal plasmacytosis is encouraged by chronic inflammation [11]. Rather from being a secondary discovery, gut microbiota dysbiosis is now understood to be a significant pathogenic contributor. Ulcerative colitis is associated with reduced microbial abundance, a rise in pro-inflammatory organisms and a drop in bacteria that make short-chain fatty acids. Changed microbial metabolites exacerbate inflammation and barrier failure by affecting epithelial energy metabolism and immune signaling regulation. The duration of illness is largely dependent on the reciprocal link between mucosal damage and dysbiosis [12].
In UC, the elevated risk of colorectal neoplasia linked to colitis is also caused by chronic mucosal inflammation. Dysregulated repair processes, oxidative DNA damage and ongoing epithelial turnover all contribute to the field cancerization effect. Dysplasia in pathology may be non-invasive and diffuse which means that inflammation leads to carcinogenesis rather than the adenoma-carcinoma mechanism in sporadic colorectal cancer [13].
To sum it up, the pathogenesis of ulcerative colitis is currently dysregulation of innate and adaptive immunity, disturbed cytokine signaling, microbial imbalance and breakdown of the epithelial barrier making the disease a complicated process. Chronic, superficial colonic inflammation brought on by these processes is accompanied by long-term consequences and distinctive histological alterations. This growing knowledge has a direct impact on the creation of focused treatments and keeps improving illness categorization and pathological evaluation [14].
Stages of Ulcerative Colitis
Mild Ulcerative Colitis: The initial symptom of the long-term idiopathic inflammatory bowel inflammation of the colon is the onset of ulcerative colitis (UC), commonly referred to as mild or early illness. At this point, inflammation begins at the rectum but is confined to the mucosal layer and could extend to the sigmoid colon. The disease is characterized by the continuous pattern without skip lesions, distinguishing UC to Crohn disease.Young individuals frequently develop acute UC, which is brought on by a confluence of immunological deficiencies, environmental variables and hereditary vulnerability [15]. Clinically, first-stage UC is characterized by mild intestinal symptoms that include rectal bleeding, urgency, tenesmus, mucus and slight elevation in the stool frequency, usually less than four bowel movements/day. This low amount of inflammation is depicted by the lack of such systemic signs as fever, acute anemia and significant weight loss. Due to the non-inflammatory symptoms, the initial UC may be confused with infectious colitis or hemorrhoidal disease, causing a postponement of the final diagnosis and treatment [16]. Early endoscopic changes consist of mild mucosal changes with no deep ulceration or spontaneous bleeding such as erythema, edema, absence of normal vascular appearance, granularity and facile friability. Histopathological examination which remains vital in the diagnosis, typically reveals basal plasmacytosis, crypt architecture distortion and augmentation of inflammatory infiltrates inside the mucous membrane and on rare inflammation of intestinal glands. Although macroscopic disease may appear benign, these microscopic changes confirm unremitting inflammation [10]. In genetically predisposed people, an incorrect immune response to luminal antigens is a pathophysiological factor of early UC. In cases of breach of the epithelial barrier, the microbial products are exposed to a higher degree, triggering the native and progressive immunity. Greater amounts of pro-inflammatory molecules such as interleukin-13 and tumor cell death factor-0 are linked to long-term inflammation and mucosal injury. Immune activation is further amplified at this early period by changes in the makeup of the gastrointestinal microbial [11]. Rapid symptom control and mucosal repair are the main goals of first-stage UC management in order to stop the illness from getting worse. The initial line therapy is the topical and oral 5-aminosalicylates that are rather effective in reducing mild distal illness into remission. Some of the more positive long-term outcomes associated with early disease intervention include a reduced risk of disease progression, dependency on corticosteroids and colorectal neoplasia. The focus of the recent treatment approaches is the early control of inflammation as a major prognostic indicator of ulcerative colitis [12].
Moderate Ulcerative Colitis
The second stage of ulcerative colitis (UC) is commonly linked with moderate disease activity between mild and severe forms. Clinically, the stage indicates that the disease has already advanced beyond the stage of superficial mucosal inflammation yet has not become fulminant or threatening to life. Patients often have objective inflammatory manifestations and more chronic symptoms which implies the further development of the disease in its initial stages or the failure to manage the disease. Moderate UC can be identified with inflammatory markers including the ones incorporated into the Truelove and Witts or Mayo scoring systems, endoscopic look and frequency of symptoms [16].
Besides increased bowel movements (four to six per day), there are usually obvious blood and mucous in the second stage. Tenesmus, urgency, nocturnal bowel movements and abdominal discomfort become increasingly apparent which significantly affecting quality of life. However, serious systemic toxicity is typically absent at this stage, although systemic symptoms including weariness, modest weight loss and low-grade fever may emerge. In contrast to moderate UC, the illness usually has a continuous pattern of involvement that extends proximally from the rectum and has more significant symptom duration [12]. More profound and widespread mucosal inflammation including crypt abscesses, elevated neutrophilic infiltration and epithelial damage are pathological features of moderate ulcerative colitis. Cytokines that promote inflammation such as interleukin-6, interleukin-13 and cells that control cancer are associated with heightened immunological stimulation.
Chronic inflammation is maintained as a result of the gut barrier becoming more and more impaired which increases permeability and prolongs antigen exposure. Even when inflammation is limited to the mucosa and submucosa if treatment is not received, persistent injury raises the chance of developing into a serious illness [17]. In compare to the milder granular appearance of early disease, endoscopic examination at this stage usually shows significant erythema, friability, erosions and superficial ulcerations. Moderate anemia raised erythrocyte sedimentation rate (ESR), elevated C-reactive protein (CRP) and elevated fecal calprotectin all of which indicate ongoing intestinal inflammation may be observed in laboratory tests. Unless problems or alternate diagnosis are suspected, imaging is usually not necessary. Assessing disease activity and ruling out infection or dysplasia still require histologic confirmation by biopsy [18].
Step-up therapy which includes higher-dose aminosalicylates, systemic or locally acting corticosteroids and steroid-dependent or refractory cases of immunomodulators or biologic agents is frequently necessary for the management of second-stage UC. Hospitalization, long-term complications like colorectal cancer and disease progression can all be avoided with early intervention at this stage. A higher relapse rate is linked to moderate UC than mild disease highlighting the significance of maintenance therapy and routine monitoring [10]. However, with the correct treatments many people experience clinical remission.
Severe Ulcerative Colitis
Overall, the third stage of ulcerative colitis is described as a severe one, systemic, extensive mucosal damage and the presence of inflammatory activity. Typically, it is determined by established indices such as the True Love and Witts criteria or the Mayo score, where patients show severe bleeding in the rectum, increased stool frequency and evidence of systemic inflammation. Suboptimal reaction to usual medication or speedy onset of illness are typical features of severe UC, which is associated with increased hospitalization, sequelae and colectomy [11]. Clinical signs of severe UC include severe stomach discomfort, tenesmus and over six bloody stools daily. Some typical symptoms that indicate a systemic inflammatory burden are fever, tachycardia, anemia, weight loss and extreme exhaustion. Long term diarrhea may also lead to electrolyte imbalances and dehydration to the patients. These symptoms considerably decrease the quality of life and often require inpatient treatment to offer close monitoring and swift treatment escalation [15].
The pathophysiological hallmarks of severe ulcerative colitis are widespread epithelium breakdown and severe diffuse mucosal inflammation. Severe architectural deformation, ulceration, extensive crypt abscesses, intense infiltration of neutrophils, lymphocytes and plasma cells are among the histologic findings. Persistent inflammation is caused by immunological responses that are dysregulated and involve cytokines including TNF-α, interleukin-1β, interleukin-6 and interferon-12. The magnitude of the inflammation puts patients at risk for consequences such toxic megacolon and perforation, even if it is still mostly limited to the mucosa [7]. Deep ulcerations, spontaneous bleeding, mucosal sloughing and a loss of the usual vascular pattern are all signs of significant tissue injury that are shown by endoscopic assessment in the third stage. Electrolyte imbalances, hypoalbuminemia, increased CRP, ESR and severe anemia are commonly seen in laboratory tests. To lower procedure risk, flexible sigmoidoscopy is frequently used in the acute situation over complete colonoscopy. The importance for early diagnosis and treatment is highlighted by the fact that severe UC is linked to major consequences such as toxic megacolon, significant bleeding, infection and an increased risk of colorectal cancer in the long run [17]. Aggressive medication is needed to treat third-stage ulcerative colitis; in most instances, intravenous corticosteroids are the first line of treatment. If steroid resistance persists, biologic medicines or small-molecule treatments may be used. Since a colectomy may save a life in cases of fulminant illness, early detection of therapy failure is crucial to preventing delays in surgical consultation. Severe UC is still linked to worse rates of morbidity and recurrence than early stages, even with advancements in medical therapy. Timely treatment, responsiveness to cutting-edge medicines and adherence to maintenance techniques meant to maintain remission and avoid complications are all critical to the long-term prognosis [18].
Fulminant Ulcerative Colitis
A fulminant and potentially fatal manifestation, the fourth stage of ulcerative colitis (UC) surpasses the clinical and pathologic severity of the usual "severe" illness. In conversely to the fulminant stage of UC which is marked by refractory inflammation such as toxic megacolon or perforation, frequent bloody stools and systemic indications of toxicity, the former stage is marked by quick development to profound systemic sickness. In the best understanding, this stage is a continuum of acute severe UC that does not respond to routine escalation of medicinal therapy, requiring emergency care and frequently surgical intervention. The excessive stool frequency (typically >10/day), persistent bleeding, noticeable abdominal distension and signs of systemic impairment are diagnostic thresholds [19]. The Clinical manifestations of fulminant UC include severe, continuous diarrhea, severe abdominal pain, profuse rectal bleeding and systemic toxicity symptoms such anemia, tachycardia, hypotension and high fever. Unlike the third (severe) stage, patients frequently experience a failed host response and overwhelming colonic inflammation which results in fast clinical deterioration even with high-dose corticosteroids and initial rescue therapy. Furthermore, unanticipated consequences such toxic megacolon which is characterized by colon dilatation and lack of peristalsis might increase the risk of sepsis and perforation; these outcomes necessitate prompt assessment and frequently surgical treatment [20]. Although UC typically mainly affects the mucosa and submucosa, the underlying pathophysiology of fulminant UC includes increased mucosal degradation and loss of epithelial integrity which can result in transmural inflammation in severe consequences. This escalation is a result of dysregulated immunological responses which include dysbiosis, barrier collapse and increased production of pro-inflammatory cytokines. These cellular and molecular processes hinder healing, increase the risk of problems such toxic dilatation and contribute to SIRS. The existing data is linked to these extreme symptoms due to long-term activation of innate immune systems and malfunction of regulatory mechanisms aimed at decreasing the degree of inflammation, although the molecular fingerprints are still under research [21]. Fulminant UC presents itself with dramatic colonic dilatation, extreme ulceration and loss of normal mucosal architecture, frequently with transmural stress revealed with imaging and endoscopy. Radiologic evidence of toxic megacolon could be air-fluid levels and an intestinal diameter exceeding 6 cm on abdominal X-ray or CT imaging and laboratory evidence of inflammatory signs e.g a high degree of leukocytosis, high CRP, metacidosis in the bloodstream and hypo-albuminemia. These outcomes and worsening of the clinical condition indicate the necessity to conduct comprehensive research and close monitoring of care. The probability of bleeding and perforation is more and this indicates the urgency of action [22].
The multimodal management of the fulminant stage includes comprehensive supportive care (fluid resuscitation, electrolyte replacement), urgent surgical referral and the potential of subtotal colectomy in case of failure of the medicinal treatment and a significant involvement of the colon. Corticosteroids IV is the initial medical intervention though up to a third of patients will be steroid-resistant and require rescue therapy using biologic (such as infliximab) or calcineurin inhibitors (such as cyclosporine); regardless of this, a high proportion of patients will still need surgical intervention. Infliximab can also reduce the colectomy rate with steroid-refractory acute severe UC, as recent meta-analyses indicate which is why new biologic strategies are required at this point. Even in the case of complications such as toxic megacolon or perforation, the prognosis remains unclear and the morbidity is significant and death is likely. As such, early detection and treatment are essential [23].
Chronic Ulcerative Colitis
Ulcerative colitis enters its fifth stage i.e., a chronic complex or end-stage stage once a person has gone through a set of severe or fulminant disease activity or when the reaction to intricate medical treatment is unsatisfactory. Long-term implications, the accumulation of tissue damage and chronic disease refractoriness, not just acute inflammatory load characterize this stage. The patients of this stage can tend to have repeated hospitalization history, use of steroids, biologic failure or surgery. History of the disease has a shift of intermittent inflammation to structural and functional long-term colon damage [24]. Although acute inflammation is not evident, people can have the following clinical manifestations: chronic diarrhea, constant rectal bleeding, stomach pain, and urgency. Extraintestinal manifestations, such as arthritis, primary sclerosing cholangitis and skin involvement are more probable in chronic disease. Functional abnormalities including reduced intestinal compliance, anorectal malfunction and bad continuance have a major effect on morbidity. Persistent complications, such as pouchitis, cuffitis, or altered bowel habits might take over the clinical presentation in a surgical patient [25].
The pathophysiological features of this stage are chronic mucosal injury, architectural deformity, fibrosis and impaired epithelial regeneration. Repeated inflammatory attacks on the colonic mucosa, including alterations of immune surveillance, dysplasia, and loss of crypts, cause permanent changes in the mucosa. Low-level, sustained immune activation facilitates carcinogenesis and a pro-inflammatory microenvironment. Compared to the previous stages, inflammation might be mild and patchy but the damage obtained will impact the normal operations of the intestines significantly [26]. A special trait of end-stage ulcerative colitis is the increased risk of developing colorectal dysplasia and cancer especially in patients with severe colitis and who have a disease of more than 810 years. Epigenetic changes, genomic instability and the advancement of the inflammation–dysplasia–carcinoma sequence are all facilitated by chronic inflammation. The complications in younger patients, related to the condition are colonic strictures, thromboembolic disease and chronic anemia. A lifetime monitoring colonoscopy would be required at this stage in order to pick up neoplastic change early [27]. Instead of considering the inhibition of acute inflammation, chronic complex UC needs to be addressed to improve the quality of life, prevent complications and control the disease. Examples of therapeutic approaches include endoscopic monitoring programs, long-term biologic or small-molecule therapy or timely referral to surgery in case medical therapy fails or dysplasia is detected. Although it adds additional functional issues, total proctocolectomy with ileal pouch–anal anastomosis is still a curative procedure for colonic illness. In order to minimize morbidity and maintain long-term results, the prognosis at this stage is dependent on early detection of problems, suitable surveillance and customized multidisciplinary treatment [28] (Figure 1).
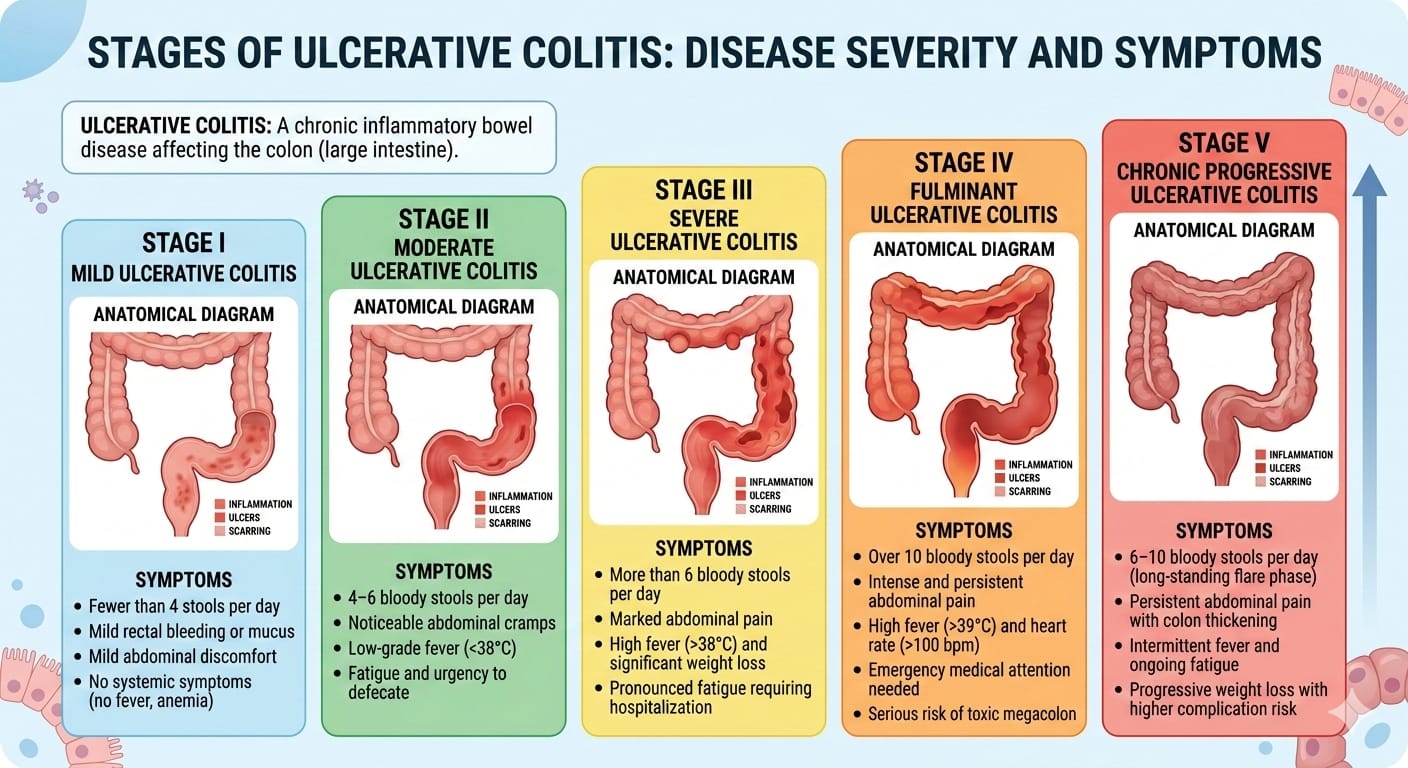
Figure 1: Evolution of Ulcerative Colitis Through Multiple Phases with Associated Symptoms
Conventional Treatment
Inflammatory bowel disease presently has no known cure and the main goals of treatment are symptom administration and averting further problems. The kind and bareness of the illness also affect how well a treatment works. Currently applicable treatments for IBD include biologics, immunomodulators, corticosteroids, amino-salicylates, surgery and lifestyle modifications. Initially, amino salicylates are used to treat moderate to severe ulcerative colitis. These substances which include balsalazide, sulfasalazine, and mesalamine, reduce inflammation by acting locally on the intestinal mucosa [29]. Their methods include antioxidant action, regulation of mucosal immunological responses, inhibition of prostaglandin and leukotriene production and compression of pro-inflammatory cytokines including TNF-α and IL-1. They are used to induce and maintain remission in mild cases and can be taken orally or rectally depends on the severity of the condition. Their advantage is constrained in moderate to harsh instances though. The majority of allergic effects are minor, although they can include headaches, gastrointestinal distress and in rare cases hepatotoxicity or nephrotoxicity [30].
For the short term, moderate to severe illness flares are managed with corticosteroids such hydrocortisone, budesonide, and prednisone. They do this by lowering leukocyte migration and preventing the generation of pro-inflammatory cytokines [31]. Because of their serious adverse effects which include weight gain, hypertension, hyperglycemia, infection risk, osteoporosis and adrenal suppression, corticosteroids are not recommended for long-term maintenance despite their great effectiveness in bringing about remission. Patients usually need to be escalated to immunomodulators or biologic therapy if they become steroid-dependent or resistant [32]. Azathioprine, 6-mercaptopurine, cyclosporine and tacrolimus are examples of immunomodulatory drugs that are mostly used as maintenance therapy for cautious to severe ulcerative colitis. These medications work by disrupting purine composite or calcineurin signaling pathways which inhibits T-cell activation and lymphocyte proliferation. Although their initial effect is delayed, they aid in maintaining remission and reducing reliance on corticosteroids. Hepatotoxicity, infection risk, bone marrow suppression, and rare cancers are among the accessible side effects that call for routine laboratory testing [33].
For individuals with moderate to severe ulcerative colitis, biologic medicines are recommended, especially if they do not respond well to traditional treatments. These include IL-12/23 inhibitors (ustekinumab), anti-integrin treatment (vedolizumab) and anti-TNF medications (infliximab, adalimumab, and golimumab). Because biologics target certain inflammatory pathways, they promote mucosal repair, lower cytokine activity and lessen immune cell trafficking to the stomach. They reduce the risk of infections, infusion responses and uncommon systemic problems but they are effective in causing and maintaining remission [34]. Particularly following biologic failure, oral small-molecule medications like Janus kinase (JAK) inhibitors (tofacitinib, upadacitinib) provide patients with moderate to severe illness more alternatives. These drugs quickly reduce symptoms by blocking intracellular signaling pathways that contribute to cytokine-mediated inflammation. Their usage necessitates a thorough risk assessment, nonetheless because of the possibility of significant infections and thromboembolic consequences. Medically resistant illness, serious consequences (toxic megacolon, perforation) or the danger of colorectal cancer are among reasons to seek surgery. The most common surgical procedure for treating colonic illness is total proctocolectomy with ileal pouchanal anastomosis (IPAA). Surgery can improve many patients' quality of life by removing the inflammatory colon but it also has complications including infection, intestinal obstruction, pouchitis and it doesn't address the underlying immunological dysregulation [35].
Medicinal Treatment
Since the beginning of time, people have advanced medicinal plants which are a gift from nature, as the basis for the conventional of pharmaceuticals. Many medicinal plants are used appropriately to treat IBD and ulcers [36].
Furthermore, a large body of research on plant extracts in recent years has occurred strong anti-inflammatory and anti-ulcer properties in both in vitro and in vivo settings.
There are two main mechanisms by which medications derived from plants may reduce intestinal inflammation: either by diminishing the exemption of pepsin and acid or by supporting cyto protection through mucosal defense mechanisms [37]. Depending on their purpose, various medications have different modes of action. These drugs balance a number of defensive (cellular mucus, mucin secretion, mucosal blood flow, bicarbonate secretion and cell turnover) and aggressive (pepsin, acid, bile salts, and H. pylori) factors, because they are natural products. The use of natural products like plants and herbal derivatives is growing among patients with ulcers and inflammation and they have few or no side effects. Several plant species that are now thought to be useful in treating inflammatory illnesses, ulcers and many other diseases. There are few plant species which are discussed below:
The Liliaceae plant A. vera is referred to as "aloe vera" globally and as "ghritkumari" in Bangladesh and India [38]. The active chemical compounds found in A. vera leaves, primarily saponins, essential amino acids (such as cysteine, alanin, arginine and histidine), anthraquinones (such as aloetic acid, aloin A and B (or collectively known as barbaloin), anthracine, anthranon, emodin, etc.), enzymes (such as alkaline phosphatase, amylase, catalase, cellulase, cyclooxidase, and lipase), hormones (such as auxin and gibberellins), minerals, chromones, sterols, carbohydrates (such as lignins and sugars), dietary fibers, protein, organic acids, lipids, and vitamins. Rural residents use water and the inner gel layer of fleshy leaves to cure ulcers [39]. By promoting its anti-inflammatory and healing properties and controlling mucus and stomach secretion, this plant offers a great deal of promise for both preventing and treating gastric ulcers. Duodenal ulcers, peptic ulcers, mouth ulcers and sore throats are just a few of the ailments that A. vera may effectively heal [40] (Figure 2).
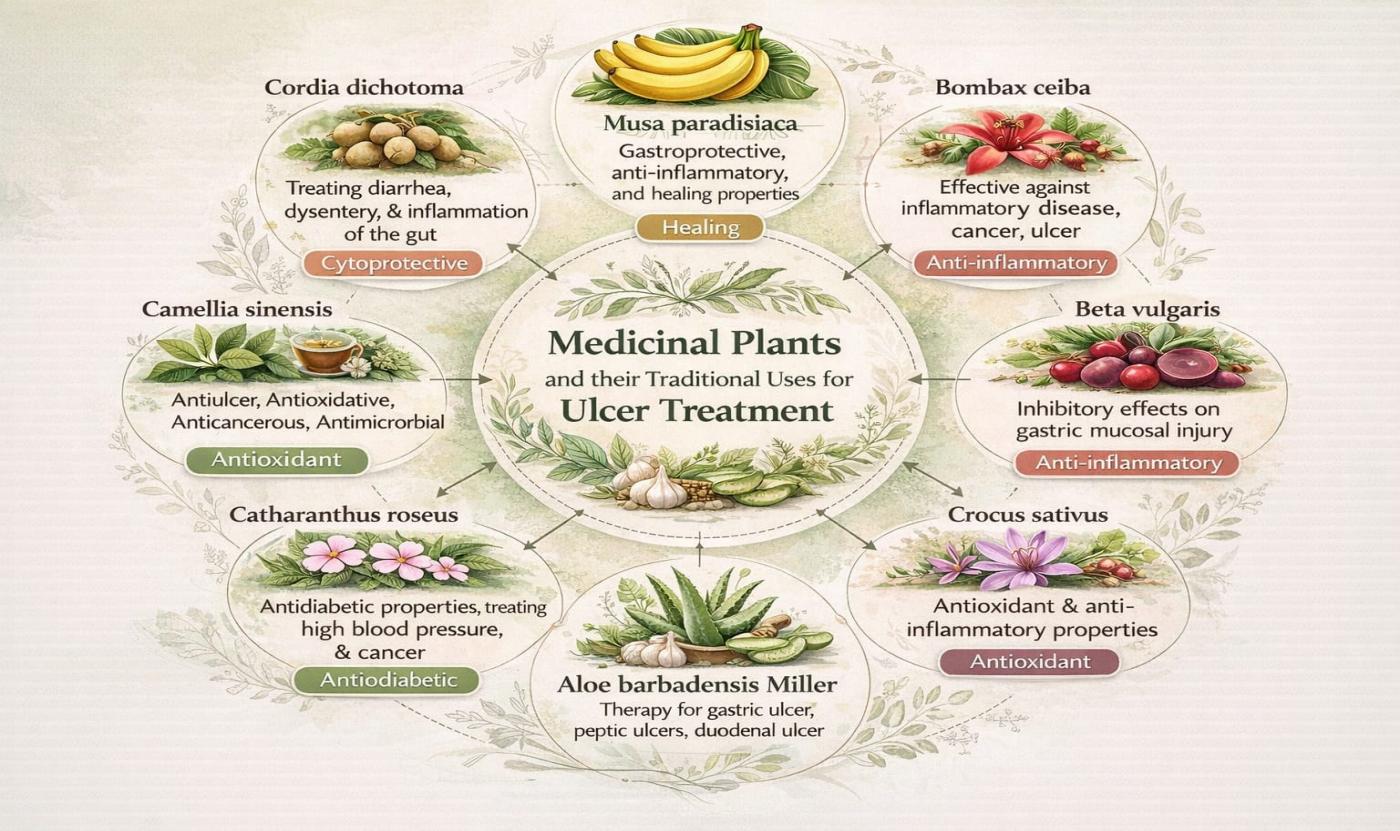
Figure 2: Medicinal Plants, their Historical use, and their Defense Mechanism against Ulcerative Colitis
The Chenopodiaceae family's Beta vulgaris is often known as "beetroot" or "sugar beet," and it's frequently eaten as a vegetable or in salads [2]. Traditionally, wounds and ulcers have been treated with the root decoction and a tiny bit of vinegar. At 200–400 mg/kg, the alcoholic root extract of Beta vulgaris dramatically reduced the ulcer score, ulcer index and overall acidity. It also preserved normal mucosa in rat models of ethanol-induced ulcer and pylorus ligation [41]. Bombax ceiba's active ingredients, which include polyphenols, tannins, alkaloids, vitamins (such as C, B3, B6, and B9), carotenoids, flavonoids, betacyanins, betaxanthins, betanin and saponins most likely have an inhibitory impact on gastric mucosal damage. Bombax ceiba is a plant that belongs to the Bombacaceae family and has a number of therapeutic uses for inflammatory conditions like cancer, ulcers, diarrhea, and microbial infections. Common flavonoids (such as isovitexin (molecular formula: C21H20O10), kaempferol 3-O-galactoside (molecular formula: C21H20O11), gallic acid (molecular formula: C7H6O5), quercetin, lupeol, tannic acid, sesquiterpenoids, naphthol, naphthoquinones, polysaccharides, anthocyanins, shamimin and alkaloids are found in B. ceiba [42]. Gynecological problems, constipation, diarrhea, piles, dysentery, sores, ulcers, inflammation and urinary infections have all historically been treated using the plant's young root paste. In mice's hot plate tests and acetic acid-induced writhing, crude plant extracts showed potent analgesic effectiveness [43] (Table 1).
Table 1: Traditional uses of Plants with their Mechanism in Ulcerative Colitis
|
Genus |
Plant name |
Traditional Use |
Part used |
Mechanism |
References |
|
Anogeissus
|
Anogeius latifolia
|
used to treat liver problems, hemorrhoids, congestion, ulcers and dysentery. |
Leaves, barks |
Scavenges free radicals (ROS), polyphenols, pro inflammatory cytokines etc |
Rahman et al. [38] |
|
Azadirachta
|
Azadirachta indica
|
inflammation, fever, ulcer, arrhythmia, protozoa and gastrointestinal disorders |
Leaves |
stimulates humoral and cellular immunological responses and increases macrophage activation to exhibit immunomodulatory effects. |
Priyanka [37] |
|
Musa |
Musa paradisiaca |
gastroprotective arthritis, cure inflammatory disorders |
Leaf, peel |
Anti- inflammatory, antioxidants properties |
Huang et al. [44] |
|
Colocasia
|
Colocasia esculenta
|
Used to cure indigestion, constipation, cancer, tumors and ulcers |
Stem, leaf, barks, seed, roots |
Antioxidant activity reduces lipid peroxidation, Mechanism of anti- inflammatory inhibits proinflammatory mediators |
Andrade et al. [45] |
|
Excoecaria
|
Excoecaria agallocha
|
Helpful for bacterial diseases, cancers, Wound healing and intestinal infections |
Seed, leaves extract |
Boost up endogenous antioxidant defense system, decrease oxidative stress |
Maan et al [40] |
|
Ginkgo
|
Ginkgo biloba
|
treat stomach ulcer
|
Seeds |
reduction in NF-κB signaling, |
Liu et al. [3] |
|
Lannea
|
Lannea coroman delica |
Anti-leprous, anti-ulcer, anti-emergence and ulcerative dyspepsia |
Stem Barks, leaves |
Blockage lipoxygenase (LOX) and cyclooxygenase (COX) pathways, potential inhibition of the NF-κB pathway |
Wang et al. [25] |
|
Poaceae |
Cymbopogon proximus |
alleviation of cramps in abdomen Spasms in digestive tract, Urinary spasm linked to kidney stones Rheumatism related discomfort |
Barks, leaf |
Control of inflammation by antioxidants, prevention of oxidative damage to renal tissue |
Moglad et al. [46] |
|
Solanaceae |
Physalis angulata L. |
Antibacterial, diarrhea, malaria, asthma |
Leaves |
Stops cytokines like IL-2, I L-6 |
Chandan et al. [46] |
|
Cordia |
Cordia dichotoma |
Medicinal use for gastrointestinal diseases, ulcer diarrhea, dyspepsia, constipation and skin infection |
Fruit, Bark, leaves |
Proinflammatory cytokines like NF-κB decreases the reduce nitic acid, formulation of prosglandins, Anti-oxidants enzymes like catalase decreases lipid production |
Subudhi et al. [9]
|
|
Crocus |
Crocus sativus |
Ulcer, anti- depressant, abdominal pain and asthma |
Whole plant |
Restrain the proinflammatory cytokines (TNF-α, IL-1β, and IL-6), decrease oxidative stress and altering the makeup of the gut microbiome to encourage the growth of beneficial bacteria |
Zhu et al. [11]
|
|
Aegle |
Aegle marmelos |
Cure cancer, ulcer diarrhea, Inflammation of the rectal cavity and peptic ulcers |
All parts of plant |
Bioactive compounds such as Flavonoid, Tannis, polyphenols control the inflammatory cytokines and suppress the oxidative stress |
Pynam and Dharmesh [39] |
|
Alpinia |
Alpinia nigra |
For Gastric ulcer |
Leaf extract |
Natural ingredients release anti-inflammatory and have analgesic properties |
Gupta et al. [13] |
|
Annona |
Annona squamosa |
For ulcer, cancer |
Whole plant |
Activity of enzymes, cellular potency used for lethal disorder and natural compounds such as tannis, flavonoids and phenolics produce the anti-inflammatory and anti-oxidants |
Ahmed et al. [5] |
|
Anthocephalus
|
Anthocephalus cadamba
|
Gastric ulcer, stomach disorder, intestinal infection |
Bark, leaf |
Restrict the gastric lesion in ulcer, reduce the acidity and role in anti- inflammation and analgesic potentials |
Ahmed et al. [5] |
|
Aristolochia |
Aristolochia indica |
Therapy for cancer and ulceration and intestinal sore |
Roots extract |
Increases B cell and induction of hyposensitive agents to control inflammation |
Ahmed et al. [5] |
|
Thespesia |
Thespesia populnea |
Cure intestinal diseases and peptic ulcer |
Roots, Fruit |
Antioxidant’s activity, reduction of swelling |
Nirmal et al. [2] |
|
Brassica |
Brassica juncea |
For ulcer colitis and inflammatory disorders |
Leaves, bark |
Reduce inflammatory cytokines enzymes, decrease oxidative stress |
El-Meligy et al. [48] |
|
Cassia |
Cassia obtusifolia |
Inflammation of colon |
Stem, bark and leaf |
Stimulation of colonic IL-6, indication of NF-κB |
Chandan et al. [47] |
|
Arctium |
Arctium lappa |
Used for gastrointestinal infection, antibacterial, Intestinal sore |
Whole plant |
Provides defense by suppression of inflammatory factors such as mucosal vascular addressin, intercellular adhesion molecule (ICAM)-1, macrophage inflammatory protein-(MIP)-2 |
El-Meligy et al. [48] |
|
Boswellia |
Boswellia serrata |
Therapy for submucosal damage, colon cancer and inflammatory diseases |
|
Restrain pro inflammatory enzymes like NF-ĸB, and leukotriene B4 (LTB4) by its antiulcerative potentials |
Ebrahimpour et al. [49] |
Camellia sinensis, is the most widely consumed beverage in the world. The main source of numerous active ingredients that have antiulcer, antioxidative, anticancer, anticarcinogenic, antiarteriosclerotic, hepatoprotective and antimicrobial properties is tea. These constituents include gallic acid, caffeine, epigallocatechin, catechins and polyphenol [13].
Cordia dichotoma, a medium-sized, evergreen, non-vascular, and non-spiny, deciduous tree, with the family Boraginaceae, is distributed throughout tropical and subtropical areas of Asia. The plant commonly referred to as Indian cherry or lasora is valued in the traditional medical practices due to the numerous medicinal applications. Phytochemical studies have shown the fruits to contain bioactive compounds, such as flavonoid (such as quercetin and kaempferol), triterpenoid (such as α-amyrin, 2-amyrin, and betulin), phenolic compounds (such as gallic acid and caffeic acid), alkaloids, glycosides, saponins and a significant quantity of muc. The fruit's moderate laxative and soothing qualities are a result of its mucilaginous texture. The anti-inflammatory and expectorant effect of the plant has been used traditionally to treat respiratory illnesses such as bronchitis, colds, coughs and sore throats. Moreover, the fruits and bark are also employed in the treatment of gastrointestinal disorders like ulcers, diarrhea, constipation and dyspepsia. The use of topical treatments of the leaves and the bark is recommended in the treatment of the skin infections and wounds. In ethnomedicine, it is also a treatment of the herb in urinary complications, jaundice and as a moderate diuretic. It also has hepatoprotective properties. These traditional claims indicate great pharmacological potential and need for more scientific confirmation as evidenced by the presence of different phytoconstituents [9].
The Bombacaceae family includes the plant B. ceiba, which has a number of therapeutic benefits against inflammatory conditions like cancer, ulcers, dysentery and microbiological infections. The medicinally active parts of B. ceiba include bark, latex, leaf, flower, seed, stem, rhizomes, thorn, stem bark, fruit and heart wood. These parts contain common flavonoids such as isovitexin (molecular formula: C21H20O10), kaempferol 3-O-galactoside (molecular formula: C21H20O11), gallic acid (molecular formula: C7H6O5), quercetin, lupeol, tannic acid, sesquiterpenoids, naphthol, naphthoquinones, polysaccharides, anthocyanins, shamimin, lupeol and alkaloids. This plant's young root paste has long been used to treat urinary tract infections, wounds, ulcers, inflammation, piles, diarrhea, constipation and gynecological issues [5].
The annual blooming plant Crocus sativus (family: Iridaceae) is grown extensively in places like Iran, India, Greece and Spain for its dried stigmas which are referred to as saffron. Its complex phytochemical profile makes it one among the most important culinary and medicinal plants. Carotenoids like crocin, crocetin, monoterpene aldehydes like safranal and the glycoside picrocrocin are the main bioactive components that give it its distinctive color, flavor and scent.
The plant also contains phenolic acids, anthocyanins, vitamins, minerals and flavonoids (kaempferol). The Ayurvedic, Unani, Persian and traditional Chinese medical traditions have traditionally made extensive use of Crocus sativus. It is considered a nervine tonic which can be used in the treatment of cognitive problems, anxiety, depression and insomnia. The herb is also commonly used to treat menstruation abnormalities e.g; amenorrhea and dysmenorrhea due to its emmenagogue properties. There is also the use of saffron as a digestive, carminative, antispasmodic and respiratory (e.g; cough and asthma). Its topical applications encompass wound healing and treating skin pigments problem [49]. The variety of pharmacological effects that have been reported on Crocus sativus can be largely attributed to its unique phytoconstituents, which include neuroprotective, anti-inflammatory, antidepressant, anticancer as well as antioxidant effects. Such findings support the long tradition of the traditional use of this plant and emphasize the potential to conduct more therapeutic research [11].
Catharanthus roseus (L.) or periwinkle of Madagascar. G. Don, is a perennial herb of Apocynaceae family that is renowned because of its excellent pharmacological effect especially in the treatment of cancer. Vincristine and vinblastine, 2 of the most therapeutically important of the over 130 known terpenoid indole alkaloids (TIAs) in C. roseus, is a Madagascar-native plant which is now widely grown in every region of the tropical and subtropical world. They have the potential to block microtubule formation and also to disrupt mitosis, which has seen these bisindole alkaloids revolutionize cancer therapy and find widespread use in the treatment of both solid and hematological cancers, such as breast cancer, Hodgkin lymphoma and leukemia. C. roseus is not only the plant with anticancer properties but also a broad spectrum of biological activity such as antidiabetic, antihypertensive, antimicrobial, antioxidant, anti-inflammatory and wound-healing activities due to its diverse phytochemical profile including alkaloids, flavonoids, saponins, tannins and phenolic compounds. The native medical practices have long been utilizing the leaves, stems, roots and blossoms among others of this plant in the treatment of the inflammatory diseases, diabetes and infections among other diseases. C. roseus has been a major subject of phytochemical, pharmacological and biotechnological research seeking to harness its entire pharmacological potential and guarantee sustainable production owing to its enormous therapeutic potential and economic significance in the pharmaceutical industry [51].
Role of Phytochemicals in Ulcer Colitis
Apigenin is a flavonoid present in Cordia dichotoma. Their traditional use such as helpful in treating gastrointestinal disease, ulcer, constipation. Intestinal inflammation and damage are mostly caused by the mucosal immune system, and cytokines are crucial in controlling inflammation. A histopathological analysis revealed neutrophil infiltration, edema, and necrosis of epithelial cells. The cause of this is elevated levels of both TNF-α and PGE2. IBD patients' intestines express a much of TNF-α. LITAF (lipopolysaccharide-induced TNF-α factor) which causes TNF-α expression in human macrophages was recently discovered to be considerably higher than controls in ileal and colonic tissue macrophages from UC patients. TNF-α is responsible for the higher PGE2 level. However, the generation of PGE2 and TNF-α as well as the gross lesion scores were considerably reduced by the isolated apigenin of C. dichotoma bark. It may have an impact on TNF-α by either preventing the activation of this proinflammatory mediator and its transcriptional regulator or preventing macrophages from producing it. Conversely, inhibition of PGE2 may occur as a result of its capacity to inhibit cyclooxygenase enzymes or may follow that of TNF-α. Amplification of the inflammatory response causes inflammatory cell infiltration which sets off pathological reactions and IBD symptoms since the gut is always in a state of regulated inflammation. According to our research, acetic acid increased colonic MPO levels, suggesting neutrophil infiltration and inflammatory system disruption. This finding has been shown in both IBD patients and animal models [52].
By preventing TNFα-induced NF-κB transcriptional activation, apigenin has anti-inflammatory properties. Because of their anti-inflammatory properties, flavonoids can help prevent cardiovascular disease and cancer. Additionally, flavonoids have been shown to suppress the production of COX-2 in epithelial cells in inflammatory circumstances. By suppressing colon MPO and improving histological characteristics, isolated apigenin from C. dichotoma bark reduced neutrophil infiltration. Oxidative stress contributes to the development and course of IBD. When endogenous defense systems are compromised, ROS assault cellular macromolecules compromising the integrity of epithelial cells and impeding mucosal healing. Apigenin of C. dichotoma bark inhibits acetic acid-induced ROS formation in this work because it has been shown to be a good antioxidant. Its capacity to inhibit free radical generation, as demonstrated in this work by restoring the redox state of the colonic mucosa, provides another explanation for this plant's anti-ulcerogenic activity [53].
The herb (family: Aristolochiaceae) has been used to treat inflammatory illnesses, ulcers and other conditions. The main classes of phytoconstituents shared by all Aristolochia species, including Aristolochia indica, are aristolochic acids and esters, aristolactams, terpenoids and flavonoids. Among them, aristolactams (molecular formula: C17H11NO4) is a Nitro phenanthrene alkaloid which are typically thought to be produced via the cyclization condensation reaction from the reduction products of aristolochic acids. It has medicinal importance for intestinal disorders and protect inner mucosal lining. Twelve aristolactams from the Aristolochia species have been identified; six of these compounds feature 3,4-methylenedioxy substitution groups. The isolated chemicals aristolactam I and hinokinin from A. indica have been shown to have anti-inflammatory properties against TNF-α and IL-6, respectively. While aristolactam I used an NF-κB independent approach, hinokinin used a nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) dependent route to demonstrate its anti-inflammatory benefits. The hyposensitive agent known as "compound 48/80" (a condensation product of N-methoxy phenethylamine and formaldehyde) which has an almost identical inhibitory pattern to synthetic anti-inflammatory medications like ketotifen fumarate was successfully inhibited by the ethanol extract of the root bark of A. indica [5] (Figure 3).
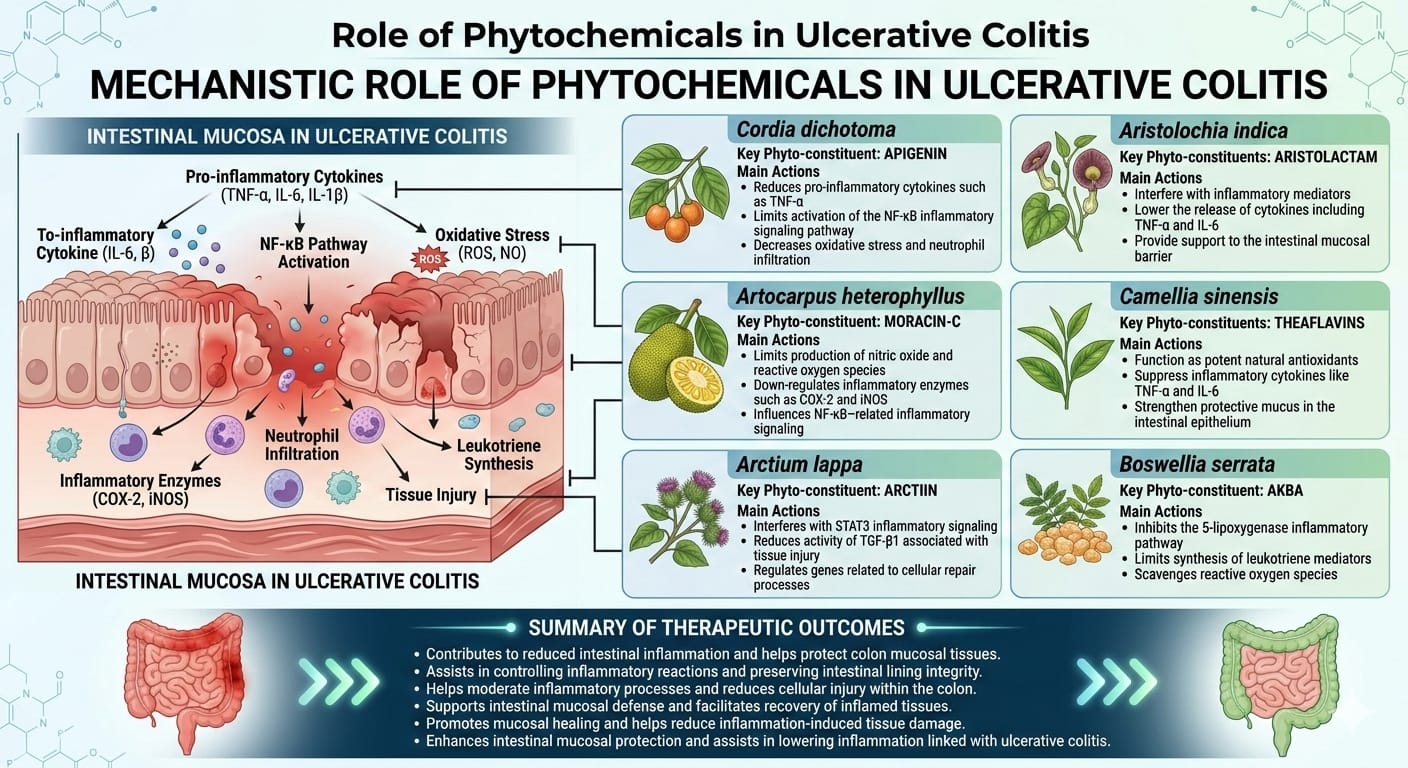
Figure 3: Phytochemical Analysis of Medicinal Plants Aimed at Inflammatory Pathways in Ulcerative Colitis
Artocarpus heterophyllus is referred to locally as "kanthal" and belongs to the Moraceae family. Young leaves combined with roots are typically helpful for skin issues, respiratory conditions, diarrhea (oral medicine) and leaf ash is given orally to cure ulcers. At a dose of 500 mg/kg, the methanolic extract of A. heterophyllus reduced the concentration of stomach acid raised the concentration of gastric pH and prevented indomethacin-induced gastric ulceration. In a different experiment, A. heterophyllus was used to isolate the natural phenolic compound Moracin-C (molecular formula: C19H18O4) is a flavoid, which has been shown to have significant anti-inflammatory effects by preventing the release of lipopolysaccharide (LPS), activated nitric oxide (NO) and reactive oxygen species (ROS) without exhibiting discernible cytotoxicity. Additionally, LPS-induced mRNA up-regulation and protein production of inducible cyclooxygenase-2 (COX-2), nitric oxide synthase (iNOS) and many pro-inflammatory cytokines (e.g., IL-1, IL-6, and TNF-α) were considerably reduced by the chemical Moracin-C. By reducing the nuclear translocation of the NF-κB p65 subunit as demonstrated by confocal microscopy and nuclear separation experiments. Moracin-C's anti-inflammatory effect was associated with the activation of the mitogen-activated protein kinases (such as p38, ERK and JNK), NF-κB pathways [5].
Table 2: Phytochemical Analysis of Medicinal Plants aimed at Inflammatory Pathways in Ulcerative Colitis
|
Plants |
Phytochemical |
Class |
Mechanism |
References |
|
Azadirachta Indica |
Nimbidin |
tetranortriterpenoid |
suppress the activity of the proton pump, H+/K+-ATPase, in the parietal cells of the stomach, slow down the production of both basal and stimulated gastric acid and down regulate the stomach's volume and overall acidity. |
(Eid et al. [56] |
|
Ginkgo biloba |
1. kaempferol 2. bilobalide |
1.flavonoid glycosides 2. Diterpene lactones |
Retrain the pro inflammatory cytokines, enhance the mucosal function Antipathy to platelet-activating factor (PAF) |
(Eid et al. [57]
|
|
Lannea coromandelica |
Morin |
Flavonoids |
Stop the stimulation of NF- κB, control nitric acid and pro inflammatory cytokines and restrict the COX2 show the decrease infection of mucosa |
Siam et al. [58] |
|
Cordia dichotoma |
Apigenin |
Flavones |
Slow down the stimulation of TNF-α and PGE2, inhibition of proinflammatory factors |
Ganjare et al. [53]
|
|
Aegle marmelos |
Aegeline |
Alkaloid (quinazoline type) |
Inhibition of proinflammatory cytokines such as:TNF-α,IL-6,block excessive immune stimulation and inflammatory striking |
(Shah and Solanki [59] |
|
Alpinia nigra |
Kaempferol |
flavonoid
|
Constrain Cytokines production, striking the NF-kB OR MAPK and defend the intestinal lining |
(Ahmed et al. [5] |
|
Boswellia serrata
|
Acetyl-11-keto-β-boswzllic acid (AKBA) |
Pentacyclic triterpenic acid |
Stop 5-lipoxygenase decrease production of leukotrein in neutrophillic granulocytes |
Suchita et al. [60] |
|
Arctium lappa |
Arctiin |
Lignans |
Prevent the cytokine pathways such as TNF‑α, IL‑1β, IL‑6 |
de Souza et al. [54] |
|
Annona squamosa |
Quercetin |
Flavanol(flavonoid) |
Blockage the level of TNF-α, IL-6, defend colonic lining, having powerful antioxidants activities |
Al-Zubaidi et al. [61] |
|
Anthocephalus cadamba |
Cadambine ne |
Monoterpenoid indole alkaloid |
Having anti- inflammatory and antioxidants properties role in gastroprotection |
(Ahmed et al. [5] |
|
Aristolochia indica |
Aristolactum |
Nitro phenanthrene alkaloid |
Modulate NF-kB factor, stops cytokines activity |
(Ahmed et al. [5] |
|
Artocarpus heterophyllus |
Moracin-C |
Prenylated flavonoid |
Restrict the lipopolysaccharide, stimulate the nitric oxide, reactive oxygen species and slow down the pro inflammatory cytokines |
(Ahmed et al. [5] |
|
Camellia sinensis |
Theaflavin |
Polyphenol |
Increases the Prostaglandin, trigger the mucosal flow of blood and bicarbonate production |
(Ahmed et al. [5] |
.
Theaflavins, which are polyphenolic phytochemicals obtained from Camellia sinensis leaves during the fermentation process of black tea, have been extensively researched for their potential to protect the gastrointestinal tract. Theaflavins use a variety of biological processes to deliver their therapeutic benefits in the treatment of ulcers. They mainly act as strong antioxidants, which protect gastric mucosal cells against oxidative damage by inhibiting lipid peroxidation and eliminating reactive oxygen species. Moreover, they exert antimicrobial effects against Helicobacter pylori, a major cause of peptic ulcers by inhibiting the growth of the bacteria, as well as preventing its adhesion to the stomach epithelial cells by blocking the production of pro-inflammatory cytokines such as TNF-a, IL-1b, and IL-6 that cause mucosal damage. Also, theaflavins provide an additional protection to the natural defenses of the stomach by increasing the amount of mucus secreted and enhancing the strength of the gastric mucosal lining that serves to protect the stomach lining against the effects of acid and pepsin. A combination of antioxidant, anti-inflammatory, antibacterial and cytoprotective activity means that theaflavins play a significant role in the prevention and treatment of stomach ulcers [5].
Altering inflammatory and cellular signaling networks, the lignan phytochemical arctiin, found in plants such as Arctium lappa could prevent and treat stomach ulcers. Arctiin, according to research inhibits the activation of the STAT3 signaling pathway by inhibiting the phosphorylation of STAT3 at the tyrosine-705 residue and significantly reduces synthesis of transforming growth factor-B1 (TGF-B1). The inhibition of STAT3 by Arctiin is beneficial in reducing inflammation and cell stress at the site of the ulcer because chronic stimulation of the STAT3 protein is associated with inflammatory response and tissue damage in the stomach mucosa [54]. Many downstream genes such as as VEGF, cyclin D1 and Bcl-xL which control cell proliferation and inflammation progression are also down-regulated by the inhibition of STAT3. Furthermore, TGF-β1 signaling decrease may help avoid excessive fibrosis during tissue repair, enabling better regulated regeneration of the stomach mucosa. Arctiin could potentially offer mucosal defense and accelerate gastric ulceration healing by preventing proinflammatory cues, fibrosis and modulating tissue injury and repair genes [55].
One of the bioactive triterpenoid compounds that was found in Boswellia serrata, acetyl-11-keto-2-boswellic acid (AKBA), has had promising therapeutic effects in the treatment of stomach ulcers. The anti-ulcer effect of AKBA is mainly due to its strong anti-inflammatory effect which inhibits 5-lipoxygenase pathway and reduces the production of leukotrienes that cause all inflammatory responses in the stomach mucosa. Additional, AKBA possesses antioxidant properties which preserve the gastric mucosa against oxidative damage as it neutralizes reactive oxygen species and inhibits lipid peroxidation of the gastric tissues. Mucosal defense is also enhanced by AKBA by stimulating mucus production and by enhancing the integrity of the gastric epithelial barrier. It can also inhibit the production of inflammatory cytokines and stimulate tissue repair by inhibiting the activation of inflammatory signaling pathways such as the NF- kB signaling pathway. Combining its anti-inflammatory, cytoprotective, antioxidant properties, AKBA prevents and treats stomach ulcers [60].
CONCLUSIONS
In summary, there are Dysregulated immunological responses, oxidative stress, ectodermal barrier failure and an imbalance in the gut microbiota are all characteristics of ulcerative colitis, a complex, chronic inflammatory disease that may result in other consequences such as colon cancer. Examples of classic therapy include amino salicylates, corticosteroids, immunomodulators and biologics, which although useful in managing symptoms and achieving remission have limitations in their long-term use due to side effects, expense and mucosal healing. In this regard, medicinal plants and their bioactive phytochemicals have demonstrated potential as supplement or alternative therapeutic means. Several plant-derived substances such as flavonoids, alkaloids, polyphenols and terpenoids have significant anti-inflammatory, antioxidant and cytoprotective effects through the regulation of cytokine synthesis, amelioration of mucosal defense and the regulation of key signaling pathways such as NF-kg B, MAPK, As evidenced by preclinical and ongoing clinical studies, these natural medicines can effectively improve overall illness outcome, heal epithelial integrity and decrease intestinal inflammation. Thus, phytotherapy might offer safer, more cost-effective and multi-targeted treatment of ulcerative colitis, but further well-thought clinical trials are needed to endorse their efficacy, safety and therapeutic normalization to be used in the long term.
REFERENCES
- Singh, G. et al. "Protective effect of saffron in mouse colitis models through immune modulation." Digestive Diseases and Sciences, vol. 67, no. 7, 2022, pp. 2922–2935. https://doi.org/10.1007/s10620-021-07163-3
- Nirmal, S. et al. "Potential of the plant Thespesia populnea in the treatment of ulcerative colitis." Pharmaceutical Biology, vol. 53, no. 9, 2015, pp. 1379–1385. https://doi.org/10.3109/13880209.2014.982302
- Liu, C. et al. "Natural products modulate cell apoptosis: A promising way for the treatment of ulcerative colitis." Frontiers in Pharmacology, vol. 13, 2022, 806148. https://doi.org/10.3389/fphar.2022.806148
- Rehman, I.U. et al. "Anti-ulcerative colitis effects of chemically characterized extracts from Calliandra haematocephala in acetic acid-induced ulcerative colitis." Frontiers in Chemistry, vol. 12, 2024, 1291230. https://doi.org/10.3389/fchem.2024.1291230
- Ahmed, S.R. et al. "Therapeutic promises of medicinal plants in Bangladesh and their bioactive compounds against ulcers and inflammatory diseases." Plants, vol. 10, no. 7, 2021, 1348. https://doi.org/10.3390/plants10071348
- Guo, M. and Wang, X. "Pathological mechanism and targeted drugs of ulcerative colitis: A review." Medicine, vol. 102, no. 37, 2023, e35020 https://doi.org/10.1097 /MD.0000000000035020
- Yuan, Y.-Y. et al. "Inflammatory caspase-related pyroptosis: Mechanism, regulation and therapeutic potential for inflammatory bowel disease." Gastroenterology Report, vol. 6, no. 3, 2018, pp. 167–176. https://doi.org/10.1093/gastro/goy011
- Nakase, H. et al. "The influence of cytokines on the complex pathology of ulcerative colitis." Autoimmunity Reviews, vol. 21, no. 3, 2022, 103017. https://doi.org/10.106/j.autrev.2021.103017
- Subudhi, R.N. et al. "Natural approaches for the management of ulcerative colitis: Evidence of preclinical and clinical investigations." Natural Products and Bioprospecting, vol. 14, no. 1, 2024, pp. 42. https://doi.org/10.1007/s13659-024-00463-x
- Kaur, A. and Goggolidou, P. "Ulcerative colitis: Understanding its cellular pathology could provide insights into novel therapies." Journal of Inflammation, vol. 17, no. 1, 2020, pp. 15. https://doi.org/10.1186/s12950-020-00246-4
- Zhu, R. et al. "The distinguishing bacterial features from active and remission stages of ulcerative colitis revealed by paired fecal metagenomes." Frontiers in Microbiology, vol. 13, 2022, 883495. https://doi.org/10.3389/fmicb.2022.883495
- Plietz, M.C. et al. "Slow and steady wins the race: A solid case for a 3-stage approach in ulcerative colitis." Diseases of the Colon & Rectum, vol. 64, no. 12, 2021, pp. 1511–1520. https://doi.org/10.1097/DCR.0000000000002113
- Gupta, M. et al. "Natural compounds as safe therapeutic options for ulcerative colitis." Inflammopharmacology, vol. 30, no. 2, 2022, pp. 397–434. https://doi.org/10.1007/s10787-022-00931-1
- Lu, Q. et al. "Natural flavones from edible and medicinal plants exhibit enormous potential to treat ulcerative colitis." Frontiers in Pharmacology, vol. 14, 2023, 1168990. https://doi.org/10.3389/fphar.2023.1168990
- Danese, S. et al. "A multicentre prospective cohort study assessing the effectiveness of budesonide MMX® (Cortiment® MMX®) for active, mild-to-moderate ulcerative colitis." United European Gastroenterology Journal, vol. 7, no. 9, 2019, pp. 1171–1182. https://doi.org/10.1177/205064619864848
- Magro, F. et al. "Third European evidence-based consensus on diagnosis and management of ulcerative colitis. Part 1: Definitions, diagnosis, extra-intestinal manifestations, pregnancy, cancer surveillance, surgery, and ileo-anal pouch disorders." Journal of Crohn's and Colitis, vol. 11, no. 6, 2017, pp. 649–670. https://doi.org/10.1093/ecco-jcc/jjx008
- Alsoud, D. et al. "Breaking the therapeutic ceiling in drug development in ulcerative colitis." The Lancet Gastroenterology and Hepatology, vol. 6, no. 7, 2021, pp. 589–595. https://doi.org/10.1016/S2468-1253(21)00065-0
- Busch, M. et al. "Investigating the role of the NLRP3 inflammasome pathway in acute intestinal inflammation: Use of THP-1 knockout cell lines in an advanced triple culture model." Frontiers in Immunology, vol. 13, 2022, 898039. https://doi.org/10.3389/fimmu.2022.898039
- AbdelMeguid, A.M.A. et al. "Modern practical management of acute severe colitis." Indian Journal of Gastroenterology, vol. 43, no. 1, 2024, pp. 78–92. https://doi.org/10.1007/s12664-024-01522-4
- Ong Ming San, E. et al. "Recent advances in the management of acute severe ulcerative colitis." Journal of Clinical Medicine, vol. 13, no. 23, 2024, 7446. https://doi.org/10.3390/jcm13237446
- Jamal, F. et al. "Acute severe ulcerative colitis (ASUC): Clinical features, initial management, and the role of advanced therapies." Biomedicines, vol. 13, no. 10, 2025, 2544. https://doi.org/10.3390/biomedicines13102544
- Kuriakose Kuzhiyanjal, A.J. and Limdi, J.K. "Management of acute severe ulcerative colitis—An update for generalist and specialist clinicians." British Medical Bulletin, vol. 151, no. 1, 2024, pp. 3–15. https://doi.org/10.1093/bmb/ldae006
- Pillay, L. et al. "Future of acute severe ulcerative colitis—A narrative review." Journal of Clinical Medicine, vol. 13, no. 24, 2024, 7723. https://doi.org/10.3390/jcm13247723
- Xu, W. et al. "Risk factors of colorectal stricture associated with developing high-grade dysplasia or cancer in ulcerative colitis: A multicenter long-term follow-up study." Gut and Liver, vol. 14, no. 5, 2019, pp. 601–608. https://doi.org/10.5009/gnl9229
- Wang, Y.-J. et al. "Intervention and potential mechanism of non-starch polysaccharides from natural resources on ulcerative colitis: A review." International Journal of Biological Macromolecules, vol. 210, 2022, pp. 545–564. https://doi.org/10.1016/j.ijbiomac.2022.04.208
- Yamamoto-Furusho, J.K. and Gutierrez-Herrera, F.D. "Molecular mechanisms and clinical aspects of colitis-associated cancer in ulcerative colitis." Cells, vol. 14, no. 3, 2025, 162. https://doi.org/10.3390/ cells14030162
- Fanizza, J. et al. "Inflammatory bowel disease and colorectal cancer." Cancers, vol. 16, no. 17, 2024, 2943. https://doi.org/10.3390/cancers16172943
- Zhou, R.W. et al. "Molecular mechanisms in colitis-associated colorectal cancer." Oncogenesis, vol. 12, no. 1, 2023, 48. https://doi.org/10.1038/s41389-023-00492-0
- Dhaneshwar, S.S. "Colon-specific prodrugs of 4-aminosalicylic acid for inflammatory bowel disease." World Journal of Gastroenterology, vol. 20, no. 13, 2014, pp. 3564–3571. https://doi.org/10.3748/wjg.v20.i13.3564
- Chapman, T.P. et al. "Withdrawal of 5-aminosalicylates in inflammatory bowel disease." Alimentary Pharmacology & Therapeutics, vol. 52, no. 1, 2020, pp. 73–84. https://doi.org/10.1111/apt.15771
- Prantera, C. and Marconi, S. "Glucocorticosteroids in the treatment of inflammatory bowel disease and approaches to minimizing systemic activity." Therapeutic Advances in Gastroenterology, vol. 6, no. 2, 2013, pp. 137–156.
- Wéra, O. and Lancellotti, P. "The dual role of neutrophils in inflammatory bowel diseases." Journal of Clinical Medicine, vol. 5, no. 12, 2016, pp. 118. https://doi.org/10.1177/1756 283X12473675
- Baldwin, K.R. and Kaplan, J.L. "Medical management of pediatric inflammatory bowel disease." Seminars in Pediatric Surgery, 2017. https://doi.org/10.1053/j.sempedsurg/2017 .10.005
- de Mattos, B.R.R. et al. "Inflammatory bowel disease: an overview of immune mechanisms and biological treatments." Mediators of Inflammation, vol. 2015, 2015, p. 493012. https://doi.org/10.1155/2015/493012
- DeLeon, M.F. and Stocchi, L. "Elective and emergent surgery in the ulcerative colitis patient." Clinics in Colon and Rectal Surgery, vol. 35, no. 6, 2022, pp. 437–444. https://doi.org/10.1002/cbdv.202200615
- Parveen, A. et al. "Challenges and guidelines for clinical trial of herbal drugs." Journal of Pharmacy and Bioallied Sciences, vol. 7, no. 4, 2015, pp. 329–333. https://doi.org/10.4103/0975-7406.168035
- Priyanka, V. "Some of the medicinal plants with anti-ulcer activity–a review." Journal of Pharmaceutical Sciences and Research, vol. 7, no. 9, 2015, pp. 772–775.
- Rahman, S. et al. "Prevention of peptic ulcer by aqueous extract of Aegle marmelos leaf in rats." IMC Journal of Medical Science, vol. 12, no. 1, 2018, pp. 11–14.
- Pynam, H. and Dharmesh, S.M. "Antioxidant and anti-inflammatory properties of marmelosin from Bael (Aegle marmelos L.); inhibition of TNF-α mediated inflammatory/tumor markers." Biomedicine & Pharmacotherapy, vol. 106, 2018, pp. 98–108. https://doi.org/10.1016/j.biopho.2018.06.053
- Maan, A.A. et al. "The therapeutic properties and applications of Aloe vera: A review." Journal of Herbal Medicine, vol. 12, 2018, pp. 1–10. https://doi.org/10.1016/j.hermed.2018.01.002
- Zhang, L. et al. "Chemistry and biological activities of processed Camellia sinensis teas: A comprehensive review." Comprehensive Reviews in Food Science and Food Safety, vol. 18, no. 5, 2019, pp. 1474–1495. https://doi.org/10.1111/1541-4337.12479
- Ranjan, S.N. et al. "Role of medicinal plants in traditional medicine system in Bihar—A review." World Journal of Pharmaceutical Research, vol. 7, 2018, pp. 1687–1701. https://doi.org/10.20959/wjpr20185-11376
- Panda, D. "Ethnobotanical study of medicinal plants in Jajpur district of Odisha, India."
- Huang, S. et al. "Dahuang Mudan decoction repairs intestinal barrier in chronic colitic mice by regulating the function of ILC3." Journal of Ethnopharmacology, vol. 299, 2022, pp. 115652. https://doi.org/10.1016/j.jep.2022.115652
- Andrade, A.W.L. et al. "Anti-inflammatory and chemopreventive effects of Bryophyllum pinnatum (Lamarck) leaf extract in experimental colitis models in rodents." Frontiers in Pharmacology, vol. 11, 2020, pp. 998. https://doi.org/10.3389/fphar.2020.00998
- Moglad, E.H. et al. "Antimicrobial and wound healing activities of certain Sudanese medicinal plants." Saudi Journal of Biological Sciences, vol. 27, no. 7, 2020, pp. 1766–1772. https://doi.org/10.1016/j.sjbs.20.05.017
- Chandan, S. et al. "Curcumin use in ulcerative colitis: is it ready for prime time? A systematic review and meta-analysis of clinical trials." Annals of Gastroenterology, vol. 33, no. 1, 2019, pp. 53. https://doi.org/10.20524/aog.2019.0439
- El-Meligy, R.M. et al. "Prophylactic and curative anti-ulcerative colitis activity and the possible mechanisms of action of some desert plants." Journal of Enzyme Inhibition and Medicinal Chemistry, vol. 30, no. 2, 2015, pp. 250–258. https://doi.org/10.3109/14756366.2014.915394
- Ebrahimpour, S. et al. "Boswellic acid improves cognitive function in a rat model through its antioxidant activity: neuroprotective effect of boswellic acid." Journal of Pharmacopuncture, vol. 20, no. 1, 2017, pp. 10. https://doi.org/10.3831/KPI.2017.20.001
- Lu, Q. et al. "Immunology of inflammatory bowel disease: molecular mechanisms and therapeutics." Journal of Inflammation Research, vol. 15, 2022, pp. 1825–1844. https://doi.org/10.2147/JIR.S353038
- Khan, A. et al. "Catharanthus roseus: A comprehensive review of its phytochemicals, therapeutic potential, and mechanisms of action." Nature Cell and Science, 2025. https://doi.org/10.61474/ncs.2024.00044
- Sharifi-Rad, M. et al. "Antiulcer agents: From plant extracts to phytochemicals in healing promotion." Molecules, vol. 23, no. 7, 2018, pp. 1751. https://doi.org/10.3390/molecules23071751
- Ganjare, A.B. et al. "Use of apigenin from Cordia dichotoma in the treatment of colitis." Fitoterapia, vol. 82, no. 7, 2011, pp. 1052–1056. https://doi.org/10.1016/j.fitote.2011.06.008
- de Souza, A.R.C. et al. "Phytochemicals and biological activities of burdock (Arctium lappa L.) extracts: A review." Chemistry & Biodiversity, vol. 19, no. 11, 2022, e202200615. https://doi.org/10.1002/cbdv.202200615
- Alfair, B.M. et al. "Arctiin inhibits inflammation, fibrosis, and tumor cell migration in rats with ehrlich solid carcinoma." Cureus, vol. 15, no. 9, 2023, e44987. doi. 10.7759/cureus.44987
- Eid, A. et al. "A review of chemical constituents and traditional usage of Neem plant (Azadirachta indica)." Palestinian Medical and Pharmaceutical Journal, vol. 2, no. 2, 2017, pp. 75–81. https://doi.org/10.59049/2790-0231.1060
- El-Medany, A. et al. "What is the possible therapeutic effect of Ginkgo biloba on gastric ulcer induced by ammonia in albino rats?" Environmental Science and Pollution Research, vol. 27, no. 20, 2020, pp. 25082–25092. https://doi.org/10.1007/s11356-020-08856-4
- Siam, N.H. et al. "Lannea coromandelica (Houtt.) Merr.: A comprehensive review of its ethnomedicinal uses, phytochemistry and pharmacological activity." Health Science Reports, vol. 9, no. 1, 2026, e71752. https://doi.org/10.1002/hsr2.71752
- Shah, B. and Solanki, N. "Exploring the bioactive properties and mechanism of Aegle marmelos in the treatment of inflammatory bowel disease through network pharmacology and a molecular docking approach." American Journal of Translational Research, vol. 17, no. 2, 2025, pp. 748. https://doi.org/10.62347/GCCV5213
- Suchita, W. et al. "A review on phytochemistry and pharmacological activities of Boswellia serrata: A natural remedy." International Journal of Pharmacognosy, vol. 8, 2021, pp. 454–461. https://doi.org/10.13040/IJPSR.0975-8232.IJP.8(11).454-61
- Al-Zubaidi, H.J. et al. "Exploring the potential protective and anti-inflammatory effects of the crude ethanolic extract of Annona squamosa Linn fruit against ethanol-mediated gastric erosion." Open Veterinary Journal, vol. 15, no. 2, 2025, pp. 795. https://doi.org/10.5455/OVJ.2025.v15.i2.28